
Ankle sprains are the most common injury in fencing. Not the most severe, but certainly the most frequent. Data collected by the International Federation over five years of competitions confirm this: roughly one out of every four injuries leading athletes to stop training or competing is an ankle sprain. Lower-limb injuries as a whole account for more than 70% of all cases.
Fencers start with an advantage: their injury risk is about half that seen in foil and sabre. But épée has its own pitfalls. Actions are longer — around 15 seconds per touch — with repeated lunges and changes of direction that place asymmetric loads on the ankle. Nearly half of all ankle sprains in fencing occur without contact with the opponent: the foot simply gives way during a technical movement.
The real problem is not the first sprain — it’s the second one
After a first sprain, the risk of recurrence increases significantly, especially if rehabilitation is incomplete or inadequate. The ankle loses part of its neuromotor control. Put simply, it becomes less able to “sense” its position and react in time when the body has to process multiple stimuli — cognitive, motor, and environmental. This deficit can persist even after the pain has gone, weeks after the injury, when the athlete already feels fully recovered.
The most common mistake in ankle rehabilitation — and in rehab in general — is focusing only on time. “Three weeks have passed, it no longer hurts, I can go back to fencing.” But the right criterion is not the calendar — it’s function. Return to play should happen when the ankle proves it is ready, not simply when it stops hurting.
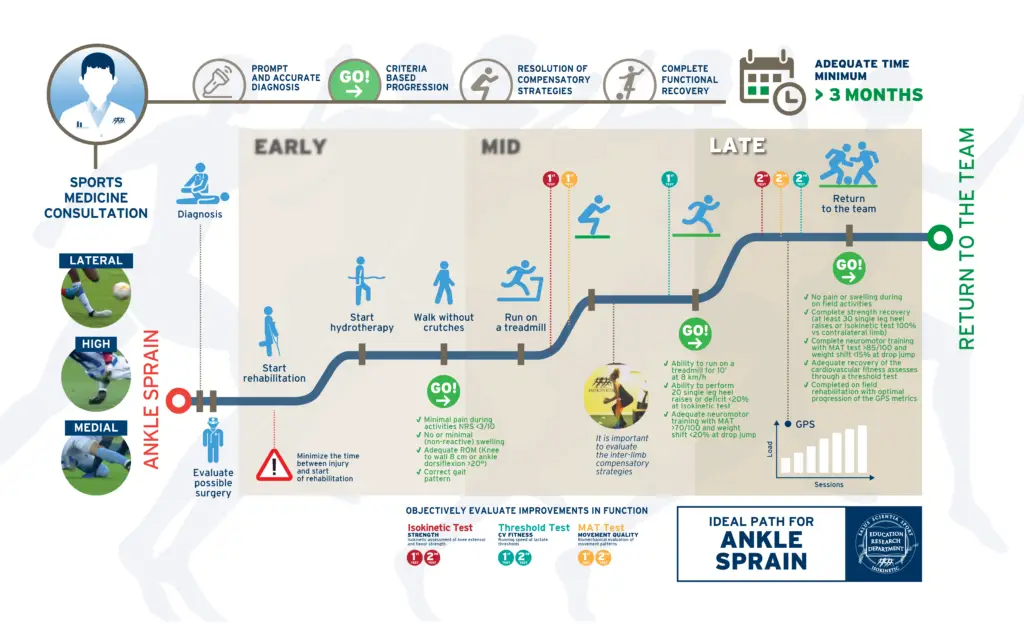
Recovery: A Stage-Based Process with Clear Progression Criteria
The rehabilitation pathway used at Isokinetic after an ankle sprain is built on scientific evidence and structured into three stages — early, intermediate, and advanced. Progression from one stage to the next requires meeting specific criteria. You do not move forward simply because “enough time has passed,” but because the ankle has achieved defined goals in mobility, strength, and movement control. The accompanying infographic illustrates the entire process in detail.
The final phase — the late stage — is the one that makes the biggest difference and is most often skipped. At this point, rehabilitation no longer focuses only on the injured ankle. The work shifts to overall movement quality, neuromotor coordination, and symmetry between the two limbs. The goal is to prevent the athlete from unconsciously developing compensatory patterns, such as overload at the knee or hip on the same side, or even on the opposite limb. These compensations can reduce performance and lay the groundwork for the next injury.
A complete, appropriate, and optimal rehabilitation program after an ankle sprain requires at least two months of work — longer than most people expect. The scientific evidence is very clear on this: shortening recovery time increases the risk of recurrence and of secondary problems affecting other joints. Athletes need to be aware of this and accept the importance of fully resolving the injury in order to prevent future ones.
The Good News: Prevention Works
Research involving large numbers of athletes is clear: neuromotor training programs — including balance exercises, stabilization work, and controlled perturbations — can reduce the risk of ankle sprains by about one third. For athletes who have already suffered a sprain, the protective effect is even greater.
✅ What can be done in practice: incorporate neuromotor control exercises into the regular training routine. Just a few minutes, performed consistently, can make a difference. Athletes who have already suffered an ankle sprain should also consider using a brace during activity. Evidence shows that both bracing and neuromotor training are effective, and they can be combined.
✅ When to seek medical advice: if pain persists and does not improve within a few days after an ankle sprain, if swelling or bruising develops, or if the ankle continues to give way during activity. A specialist evaluation — including ultrasound and, when necessary, X-rays — can assess the true condition of the ligaments and bones and help establish a rehabilitation pathway guided by objective criteria.
An ankle sprain is not just bad luck. It is a manageable and preventable injury — provided the first episode is not underestimated, the rehabilitation process is respected, and “it doesn’t hurt anymore” is not mistaken for full recovery.
Medical Doctor, Specialist in Physical and Rehabilitation Medicine
Medical Consultant at Accademia Scherma Marchesa
Isokinetic Medical Group – Turin


