
Tear, strain, pull, overload: what is the difference? During a World Cup the same incident — a midfielder leaving the pitch with a hand on the back of his thigh — is described in different words, words that shift in meaning from one dressing room to the next and from one bulletin to the next. Only one distinction matters: whether or not there is a lesion of the muscle fibres.
This is the distinction sports traumatology adopted to move past the ambiguity. An international survey showed wide variation in how the terminology is used, with the greatest inconsistencies around the word «tear». From it came the Munich consensus statement, which replaced the traditional vocabulary with a reproducible system (Mueller-Wohlfahrt, British Journal of Sports Medicine, 2013).
Two kinds of muscle problem, one question to clarify the picture
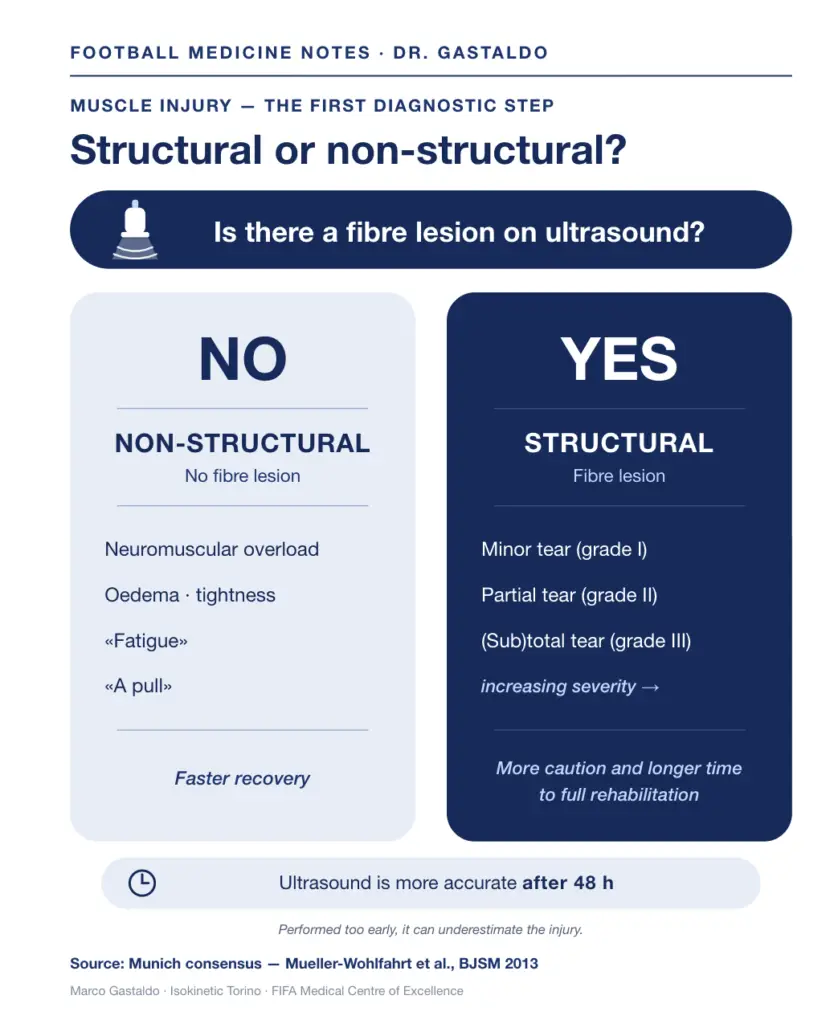
The system rests on a simple distinction. Indirect muscle injuries — those without a direct blow to the muscle — fall into two families according to one key criterion: the presence or absence of macroscopic damage to the muscle fibres.
On one side are the functional disorders, or non-structural injuries: oedema, neuromuscular overload. There is no macroscopic fibre damage. This category covers many of the conditions tradition calls «fatigue», «tightness», «a pull».
On the other side are the structural injuries: partial tears and (sub)total tears, with macroscopic evidence of fibre disruption. A grade I injury corresponds, in this system, to a minor partial tear: it is a structural injury in full, with anatomical damage and torn muscle fibres, simply of limited extent.
For clear communication — between athlete and doctor, technical staff and doctor — two categories are enough: there is fibre damage, or there isn’t.
Why it matters to everyone
Muscle injuries account for more than 30% of all injuries in professional football, with around fifteen episodes a season in a 25-player squad (Ekstrand, American Journal of Sports Medicine, 2011).
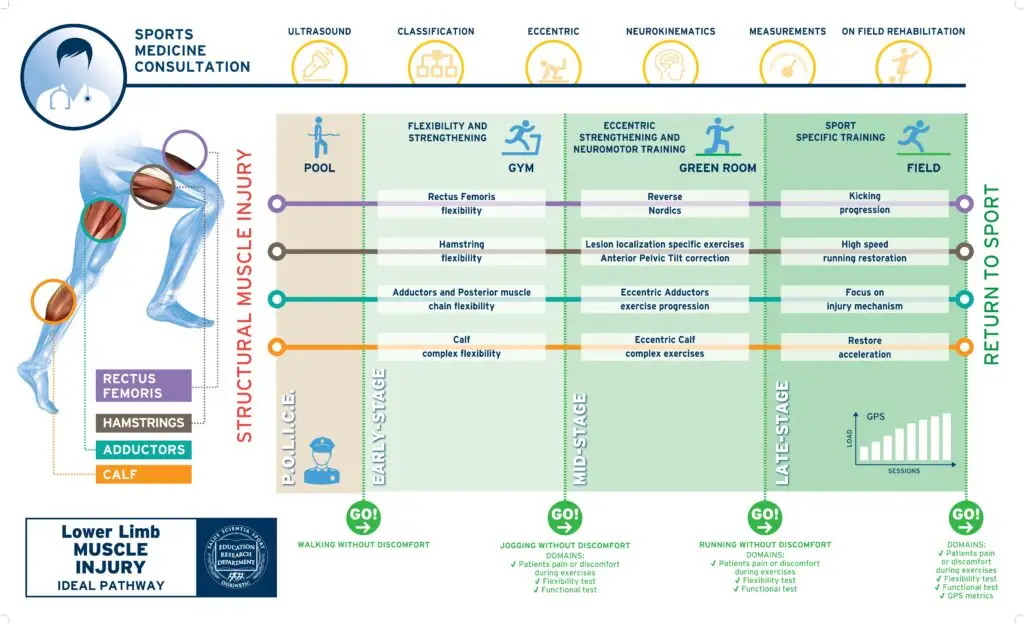
In every major tournament they are the leading cause of absence, and the 2026 World Cup in Canada, the United States and Mexico is no exception. The sites are almost always the same: hamstrings, adductors, quadriceps, calf.
Recurrence is the central problem. In studies on professional football the rate of re-injury to the hamstrings sits, depending on the study, between roughly 15% and 35%.
Reducing the number of injuries means, above all, reducing recurrences — still too many.
The same word, different outcomes
Two players with what is called, pitchside, the same «tear» can follow very different paths: one returns in three weeks, the other in two or three months, with a higher risk of re-injury. The difference often lies not in the size of the damage within the muscle belly, but in which structure is involved.
A muscle is not made of fibres alone. Running through it are intramuscular tendons, aponeuroses and fasciae: connective tissues with different architecture and function. A recent nomenclature proposes describing an injury not only by site and extent, but by the type of connective tissue involved, because tendon, aponeurosis and fascia carry distinct clinical implications (Pedret, Sports Medicine, 2025).
The clinical data follow this logic. In elite athletes, connective-tissue involvement detected on ultrasound is associated with longer return-to-play times, particularly when the connective tissue is disrupted (Renoux, Journal of Science and Medicine in Sport, 2019). In professional football, hamstring injuries involving the intramuscular tendon have shown a longer return to full training — 36 versus 24 days — and a higher recurrence risk (Shamji, BMJ Open Sport & Exercise Medicine, 2021).
What ultrasound shows

Musculoskeletal ultrasound, in expert hands, shows whether there is fibre damage and, above all, distinguishes the structures involved: muscle alone, or muscle and connective tissue (Palermi, British Journal of Sports Medicine, 2025). It is an accessible, repeatable, dynamic and immediate examination; in professional settings it sits alongside MRI, but in everyday practice it is often the first and main tool.
Its value goes beyond diagnosis. It answers not only the question «is there an injury?» but the next one — «what is injured?» — which guides prognosis and rehabilitation.
A practical point worth remembering: the examination is more informative from 48 hours after the event. Performed too early, when the haematoma and oedema have not yet organised, it can underestimate the injury. A negative scan very early on does not, on its own, rule out structural damage.
What to do, in brief
In the acute phase the sound principle is protection for as long as needed, followed soon by graded, controlled loading. Before a medical diagnosis, do not apply heat or massage the injured muscle: this can worsen the grade of the injury.
Rest means relative rest, not immobilisation, which beyond the first few days slows recovery. Anti-inflammatories are not recommended routinely, because they may interfere with tissue healing and, in the early phase, promote bleeding.
Progression matters more than the calendar. Rehabilitation based on functional criteria generally means a return slightly slower than fixed, time-based schedules, but produces fewer re-injuries (Mendiguchia, Medicine & Science in Sports & Exercise, 2017).
A few days saved on the calendar are not worth one re-injury.
It helps to separate the goals: lengthening-load work speeds the return, while trunk strengthening and agility work reduce the risk of recurrence. These are different aims, and they call for different exercises.
A note on the more debated treatments. For muscle, to date, the evidence does not support biological shortcuts: controlled studies show no consistent benefit of PRP on return or recurrence. Recovery runs through graded, criteria-guided loading that brings the player to test their sporting movement with a kinetic chain that is functional, elastic, strong and coordinated.
In summary
Behind different words — tear, strain, pull, overload — lies a single starting question: is there fibre damage or not? And, when there is fibre damage and the injury is structural, a second question often decides the path: which structure is involved, muscle alone or also the connective tissue? Musculoskeletal ultrasound, read with method and used by the specialist to guide the rehabilitation pathway, helps bring the athlete to the fullest possible functional recovery and the safest possible return to play.
Medical Doctor / Physical Medicine and Rehabilitation Medicine
Isokinetic Turin
FIFA Medical Centre of Excellence


